

Tuesday, September 30, 2025
Contouring for Thoracic Cancer
Faculty:
- Pooja Karukonda - Radiation Oncologist, Duke Cancer Institute
- Daniel Gomez - Director, Thoracic Radiation Oncology; Vice Chair of Clinical Operations, Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center
Review the case description and images below.
Case Description
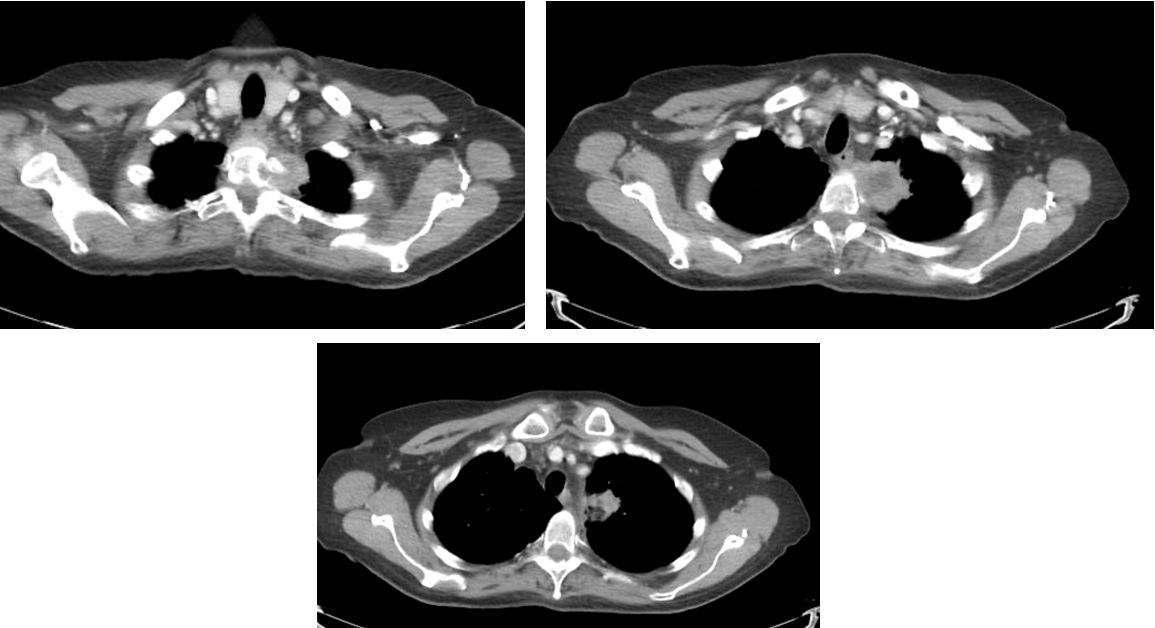
- 75 y/o woman who presented with back pain. On further workup found to have LUL mass with invasion into the vertebral body at T2.
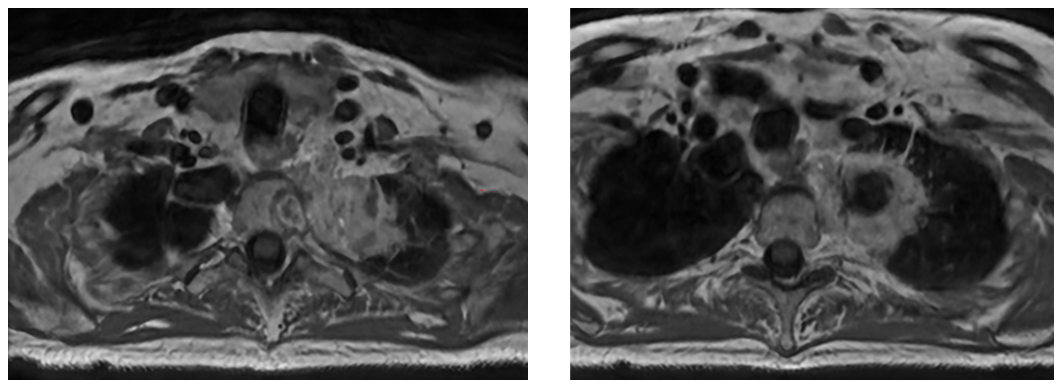
- MRI confirmed vertebral body invasion.
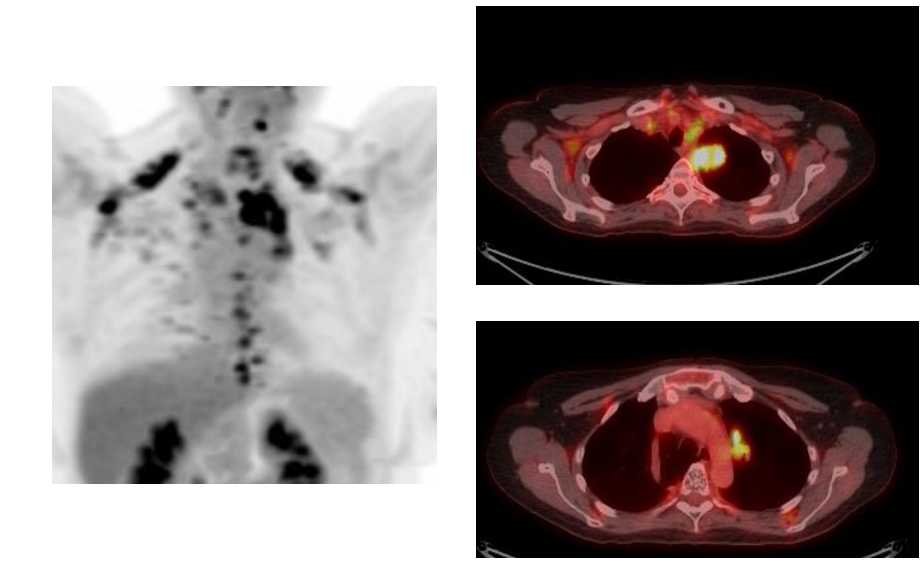
- PET images suspicious for mediastinal lymphadenopathy (SUV 3.5-5.0) and left hilum (SUV 11.0) but EBUS negative for malignancy in levels 4L, 4R, 7, 10L, and 10R.
- Patient being referred for definitive chemoRT.
Imaging
CT Images
PET Scan
MRI Scan
Contouring Questions
- Cover LN?
- Cover vertebral body?
- Simulation approach?
- Margins?
- Imaging and alignment?
Ways to Contour
Alternative 1
Alternative 2
Which volumes are the most appropriate?
A. LUL primary tumor with margin, no LN and limited vertebral body inclusion
B. LUL primary tumor + hilar LN, with inclusion of entire vertebral body and left-sided pedicle/process/lamina
C. LUL primary tumor and limited vertebral body inclusion + hilar/mediastinal lymphadenopathy
Faculty Follow Up
Answer: B
There are several potential approaches to this case. Given that the mass extends into the vertebral body and the T2 neural foramen, with unclear borders, the International Spine Radiosurgery Consortium consensus guidelines were utilized, with inclusion of the ipsilateral neural foramen and vertebral body substructures. Choices A and C are too limited with respect to vertebral body coverage, and actually appear to miss gross disease. A thin-slice MRI scan was used for treatment planning and a spinal cord PRV was utilized to ensure appropriate coverage with adequate sparing of the spinal cord.
The second major question is whether to cover the left hilum and the mediastinum. Given that the EBUS was negative, it would be reasonable to omit the entire mediastinum. However, in this case, the decision was made to cover the ipsilateral hilum given the strong avidity in the left hilum and the proximity of the mass to the left hilum, this region was covered as well.