

Saturday, September 27, 2025
Contouring for Gynecologic Cancer
Faculty:
- Jenna Kahn, MD - Radiation Oncologist, Kaiser NW Permanente
- Kevin Albuquerque, MD - Professor and Chief of Gynecological Radiation Oncology Service, Simmons Comprehensive Cancer Center, UTSW Radiation Oncology
Review the case description and images below.
Case Description
76 yr old female with stage IVA cervical squamous carcinoma with PA and right pelvic nodes, mesorectal pelvic nodes as well as right hydronephrosis, bilateral parametrial involvement and rectal wall invasion without a definite fat plane at the lower cervical mass. Definitive chemoradiation with cisplatin, immunotherapy and radiation was recommended after a multidisciplinary discussion.
Figure 1: PET/CT with mesorectal invasion and parametrial invasion
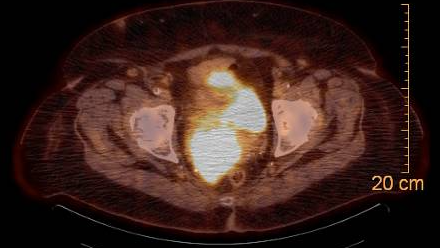
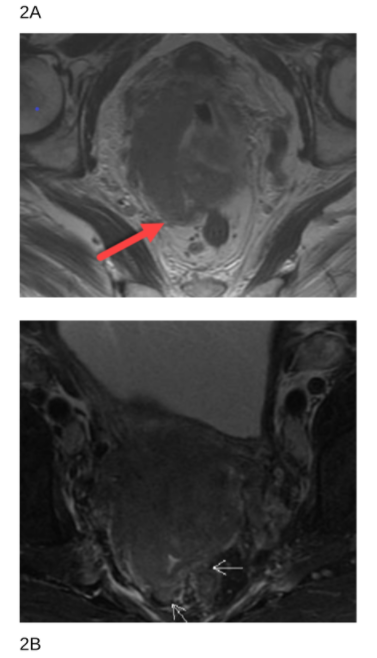
Figure 2A. and 2B. MRI images with mesorectal invasion, arrow pointing toward posterior invasion.
Click the play button to view the image series.
How would you contour this patient?
A. Uterus
B. Parametria + Cervical Tumor
C. Mesorectum + Parametria + Cervical Tumor
D. Mesorectum + Parametria + Cervical Tumor + Uterus
Faculty Follow Up
ANSWER - D. Mesorectum + Parametria + Cervical Tumor + Uterus
The inclusion of the mesorectum in clinical target volumes for cervical cancer radiation therapy remains an area of some variability and debate, particularly in the context of intensity-modulated radiation therapy (IMRT). The most recent consensus guidelines, as updated by Fields et al. (2025) in Practical Radiation Oncology, highlight that while there is substantial agreement among experts, the majority include the entire mesorectum in the CTV and accept a higher dose to the rectum - in the situation of mesorectal fascia invasion. In cases with rectal or mesorectal involvement (including involvement of mesorectal lymph nodes), most experts would cover the entire mesorectum in the CTV. This must be balanced against increased rectal dose and hence these patients who will have the mesorectum included should be carefully selected. The addition of MRI and PET imaging has helped to increase CTV volumes with more precise targeting and contouring [1].
The American Society for Radiation Oncology (ASTRO) clinical practice guideline states that mesorectal coverage may be required in select cases, specifically when there is direct rectal invasion or posterior uterosacral ligament involvement, but it is not routinely included for all patients [2]. This selective approach is based on the risk of local extension and the need to balance tumor control with minimizing toxicity.
In this case the parametria was also included given parametrial extent and involvement. Studies have shown that when parametria is involved, underdosing this region particularly in the uterosacral space increases the risk of pelvic failure [3].
In summary, routine inclusion of the mesorectum in cervical cancer radiation therapy is not universally recommended; it is reserved for cases with posterior disease extension. Parametria involvement should be assessed and included with boosting the area to allow for adequate coverage and local control. Consensus guidelines reinforce the need for individualized planning, especially in complex or advanced cases, and underscore the importance of multimodality imaging to inform CTV delineation.
HOW DO YOU DO IT
For the delineation of the mesorectum, the best approach is to follow the guidelines from the rectal cancer contouring atlas [4] which states that the mesorectum (space) extends from the rectosigmoid to the pelvic floor. In general, the full length of the rectum should be included, and every effort should be made to spare the anal canal.
A diagrammatic representation of the mesorectal space (in yellow) is shown in Figure 1 below [5].
Figure 1
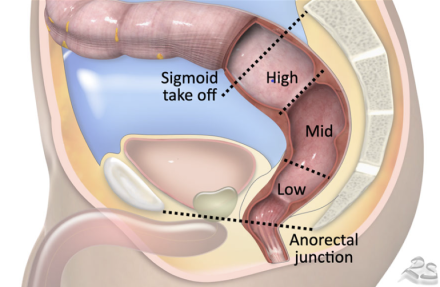
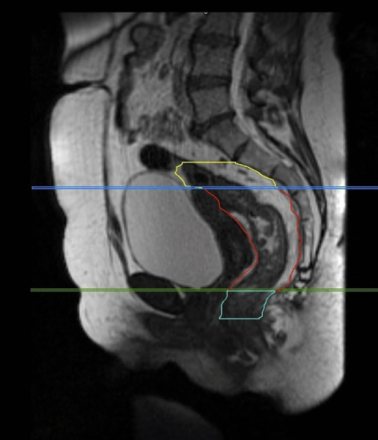
FIGURE 2 from Boldrini et al [7] showing the sagittal view of mesorectal space (in red outline) that is generally included in the target
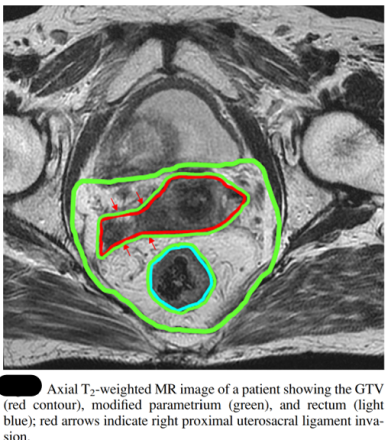
The IMRT consensus atlas by Lim et al shows the axial view of this mesorectum incorporated into the parametria below. (figure 3). The entire mesorectum is included here (green) because of the tumor involvement of the right uterosacral ligament (shown by arrows) This is best seen on MRI but can also be seen on a good contrast CT simulation [8].
Figure 3
References
1.Fields EC, Bosch WR, Albuquerque KV, et al. Consensus Guidelines for Delineation of Clinical Target Volumes for Intensity Modulated Radiation Therapy for Intact Cervical Cancer: An Update. Practical Radiation Oncology. 2025 Mar-Apr;15(2):171-179. doi:10.1016/j.prro.2024.11.004.
2. Chino J, Annunziata CM, Beriwal S, et al. Radiation Therapy for Cervical Cancer: Executive Summary of an ASTRO Clinical Practice Guideline. Practical Radiation Oncology. 2020 Jul - Aug;10(4):220-234. doi:10.1016/j.prro.2020.04.002.
3. Chao KS, Williamson JF, Grigsby PW, Perez CA. Uterosacral Space Involvement in Locally Advanced Carcinoma of the Uterine Cervix. International Journal of Radiation Oncology, Biology, Physics. 1998;40(2):397-403. doi:10.1016/s0360-3016(97)00577-4.
4. Myerson RJ, Garofalo MC, El Naqa I, Abrams RA, Apte A, Bosch WR, Das P, Gunderson LL, Hong TS, Kim JJ, Willett CG, Kachnic LA. Elective clinical target volumes for conformal therapy in anorectal cancer: a radiation therapy oncology group consensus panel contouring atlas. Int J Radiat Oncol Biol Phys. 2009 Jul 1
5. Radiology assistant ( https://radiologyassistant.nl/abdomen/rectum/rectal-cancer-mr-staging-1)
6. Cordero-Gallardo F, Lee Burnett O 3rd, McNamara MM, Weber TM, Zarzour J, Bae S, Jang S, Barrett OC, McDonald A, Kim RY. Incidence of mesorectal node metastasis in locally advanced cervical cancer: its therapeutic implications. Int J Gynecol Cancer. 2019
7. Boldrini, L., Chiloiro, G., Cusumano, D. et al. Mesorectal motion evaluation in rectal cancer MR-guided radiotherapy: an exploratory study to quantify treatment margins. Radiat Oncol 18, 4 (2023). https://doi.org/10.1186/s13014-022-02193-1
8. Lim K, Small W Jr, Portelance L, Creutzberg C, Jürgenliemk-Schulz IM, Mundt A, Mell LK, Mayr N, Viswanathan A, Jhingran A, Erickson B, De los Santos J, Gaffney D, Yashar C, Beriwal S, Wolfson A, Taylor A, Bosch W, El Naqa I, Fyles A; Gyn IMRT Consortium. Consensus guidelines for delineation of clinical target volume for intensity-modulated pelvic radiotherapy for the definitive treatment of cervix cancer. Int J Radiat Oncol Biol Phys. 2011 Feb